REBOOT: the trial reshaping cardiology and cementing the CNIC’s place as a driver of new clinical practice




For decades, the routine prescription of beta-blockers after myocardial infarction has been one of the cornerstones of clinical cardiology—an unquestioned recommendation embedded in international guidelines and applied daily in hospitals around the world. Today, that long-standing certainty is beginning to crack, thanks to the REBOOT clinical trial—an ambitious CNIC-led international study that is already reshaping medical practice and redefining the future of clinical guidelines.
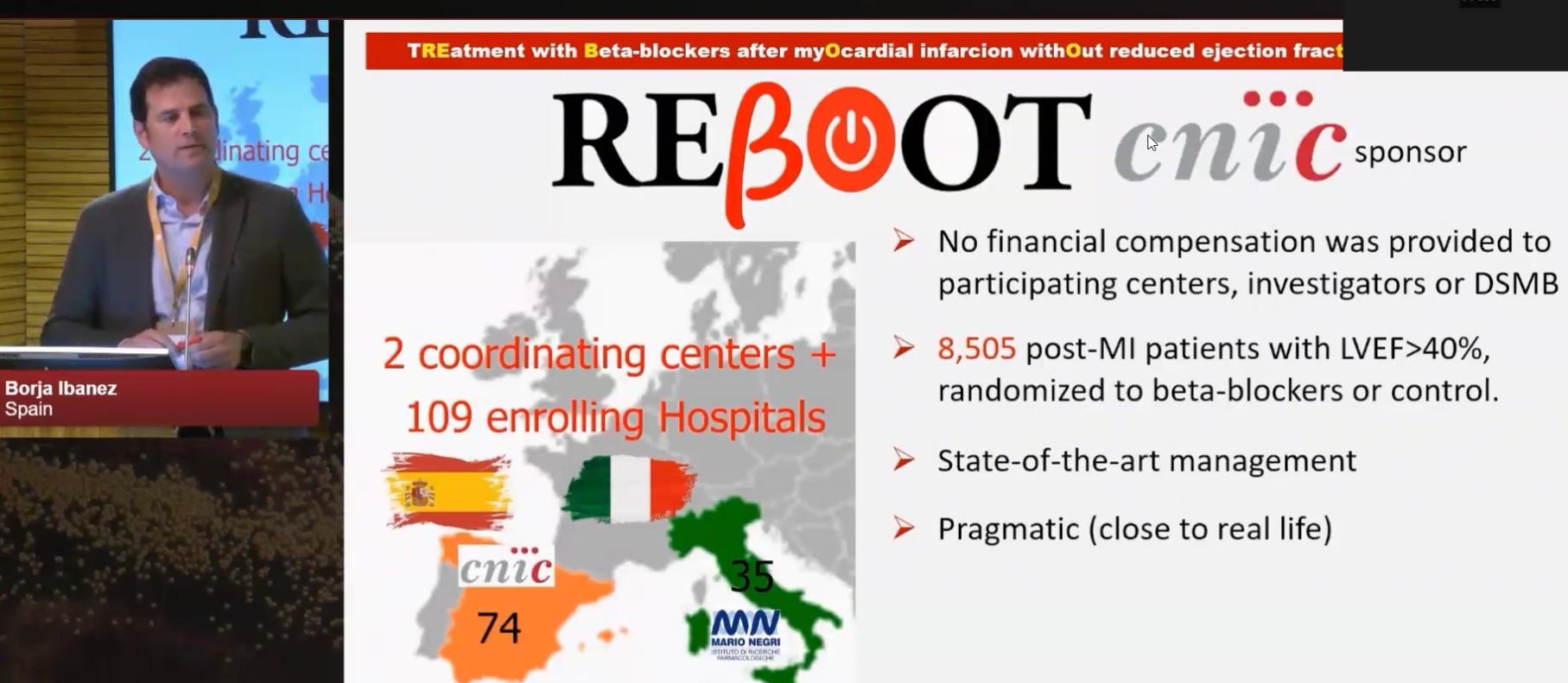
The study was led by CNIC Scientific Director Dr. Borja Ibáñez, who combines this role with work as a cardiologist at Hospital Universitario Fundación Jiménez Díaz and a group leader in the Spanish cardiovascular research network (CIBERCV). “Until now, more than eight out of every ten patients recovering from an uncomplicated heart attack have been discharged on beta-blockers, but REBOOT is set to change the treatment of these patients worldwide,” said Dr. Ibáñez. “The results of REBOOT represent one of the most significant advances in the therapeutic strategy for acute myocardial infarction in recent decades.”
REBOOT (Treatment with Beta-Blockers after Myocardial Infarction without Reduced Ejection Fraction) enrolled 8,505 patients who had a myocardial infarction but maintained ventricular function. More than 500 researchers participated voluntarily in the study, working at 109 hospitals across Spain (74) and Italy (35). The Italian arm was coordinated by the Mario Negri Institute in Milan, under the leadership of cardiologist Roberto Latini, through a collaboration agreement with the CNIC.
Participants were randomly assigned to receive or not receive beta-blockers after hospital discharge. All other components of current standard-of-care therapy were maintained, and patients were followed for a median of nearly four years.
Although generally considered safe, beta-blockers can cause side effects such as fatigue, bradycardia (low heart rate), and sexual dysfunction.
Each year, more than 2 million people in Europe have a heart attack, including around 70,000 in Spain. Traditionally, more than 80% of these patients have been discharged on beta-blockers—a practice that the REBOOT trial results call into question.
After a myocardial infarction, patients are typically prescribed multiple medications, and this complex treatment plan can make adherence difficult, explained Dr. Ibáñez. “Beta-blockers were incorporated early into standard heart attack treatment because, at the time, they significantly reduced mortality. Their benefit was linked to reduced cardiac oxygen demand and the prevention of arrhythmias. But therapies have evolved dramatically over the past 40 years. Today, occluded coronary arteries are reopened rapidly and systematically during a heart attack, and this has drastically reduced the risk of serious complications such as arrhythmias. In this new context—where the extent of cardiac damage is smaller—the need for beta-blockers is no longer clear. While we routinely test new drugs, it is far less common to rigorously examine whether long-established treatments can be withdrawn.”
The REBOOT results, published in The New England Journal of Medicine and presented at the European Society of Cardiology Congress in Madrid in August 2025, are unequivocal: in this group of patients, long-term beta-blocker therapy does not reduce mortality or the incidence of new cardiovascular events.
Xavier Rosselló, CNIC researcher, cardiologist at Hospital Universitario Son Espases in Mallorca, and one of the leaders of both the REBOOT trial and a supporting individual patient–data meta-analysis—published simultaneously in The Lancet—explained: “Taken together, these two studies provide compelling evidence that post-infarction patients with fully preserved contractile function—an ejection fraction above 50%—do not benefit from beta-blockers, whereas those with moderate or greater dysfunction—below 50%—do.”
“It is a clear message for the medical community,” said Ibáñez. “This is not about indiscriminately withdrawing treatment, but rather about identifying which patients truly benefit and which do not.”
A collaborative effort with global impact
REBOOT is not an isolated study. Its conclusions, initially supported by the meta-analysis published simultaneously in The Lancet, were subsequently reinforced by a much larger international collaborative meta-analysis in The New England Journal of Medicine.
Presented at the American Heart Association Congress in New Orleans in November 2025, the larger meta-analysis integrated data from nearly 18,000 patients across several contemporary randomized clinical trials. The results confirm that beta-blockers do not reduce the risk of death, recurrent infarction, or heart failure after an acute myocardial infarction in patients whose cardiac contractile function is normal.
Dr. Ibáñez, principal investigator of the meta-analysis and one of its four senior investigators, explained that the study analyzed individual patient data from all contemporary trials in this setting: REBOOT (Spain and Italy), REDUCE-AMI (Sweden), BETAMI (Norway), DANBLOCK (Denmark), and CAPITAL-RCT (Japan). All included patients had survived a myocardial infarction while maintaining normal left ventricular function (left ventricular ejection fraction ≥50%), indicating preserved cardiac performance.
The message is consistent: beta-blockers are no longer necessary after myocardial infarction in patients without ventricular dysfunction.
Dr. Ibáñez emphasized, however, that “beta-blockers remain an essential therapy for other patient groups, such as those with reduced left ventricular ejection fraction (<50%) after infarction or those with other conditions such as chronic heart failure or cardiac arrhythmias.”
He also stressed that “these results do not mean that patients have been treated incorrectly until now, but rather reflect the profound improvements in heart attack management in recent years, which mean that beta-blockers are no longer required in this specific context.”
For Dr. Valentín Fuster —CNIC General Director, President of the Mount Sinai Fuster Heart Hospital, and investigator in the REBOOT trial—the value of REBOOT goes beyond the drug itself. “This trial represents exactly the kind of research the CNIC should be leading: clinical studies that address a relevant question, are designed with rigor, and ultimately change medical practice internationally.”
Dr. Fuster also highlighted the symbolic importance of the project: “It is rare for a public Spanish research center to lead a trial capable of challenging long-standing clinical recommendations. REBOOT shows that Spanish research can help set the global scientific agenda.”
Sex differences: a critical variable
One of the most relevant secondary analyses derived from REBOOT, published in the European Heart Journal, introduced sex as a crucial variable. The study showed that women with preserved cardiac function who receive beta-blockers after a heart attack have a worse prognosis than those who do not receive them.
“For years, we have treated men and women as though they respond identically to therapy,” said Dr. Rosselló. “REBOOT reminds us that evidence must be analyzed through a sex-specific lens.”
“Although women in this meta-analysis experienced more adverse events when treated with beta-blockers—something we had already observed in REBOOT,” explained Dr. Ibáñez, “this difference was not large enough to reach statistical significance. This may reflect differences in drug–sex interactions between southern and northern Europe, or other factors. In any case, it is reassuring that the potential adverse effect observed in a small subgroup of women does not appear to be consistent when all trials are analyzed together.”
Dr. Fuster noted: “We have long studied sex differences in cardiovascular disease. We already knew that disease presents differently in women and men, and this study significantly advances our understanding by showing that responses to medication are not necessarily the same. This work should help drive the much-needed sex-specific approach to cardiovascular disease.”
According to Rosselló, these findings reinforce the need for increasingly individualized therapeutic decisions: “It is not enough to know that a patient has had a heart attack; we must understand their biological and clinical profile—and now also their sex—to optimize treatment.”
Dr. Ibáñez emphasized that the CNIC is committed to studying sex differences in the patterns of cardiovascular disease and treatment responses.
From evidence to clinical guidelines
The impact of REBOOT is already being felt. CNIC-led studies have been cited as key references in the development of new European clinical practice guidelines—a decisive step in translating trial results into real-world changes in patient care.
“Changing a clinical guideline is probably one of the greatest achievements in medical research,” said Fuster. “It means the evidence is so strong that it forces us to rethink how we treat millions of patients.”
A new role for the CNIC
Beyond beta-blockers, REBOOT symbolizes a deeper transformation for the CNIC, acting as a catalyst for clinical trials that challenge dogma and redefine standards of care. A model of translational research that connects the laboratory, the hospital, and clinical guidelines.
“REBOOT represents a turning point,” concluded Rosselló, “not only in how we treat myocardial infarction, but in how we view the contribution of Spanish clinical research.”
In a healthcare landscape that increasingly demands decisions grounded in robust evidence, the REBOOT trial confirms that the cardiology of the future is already being written—and that the CNIC occupies a central place in that story.
As Dr. Fuster summarized, “This study joins other landmark trials coordinated by the CNIC—such as PESA, SECURE, and DapaTAVI—that are reshaping clinical practice worldwide.”
Today, the CNIC stands among the research centers with the greatest global influence on the diagnosis and treatment of cardiovascular disease.



